Good prospects:
Latest Regulatory Filings for SP5
Companies with the best and the worst fundamentals.
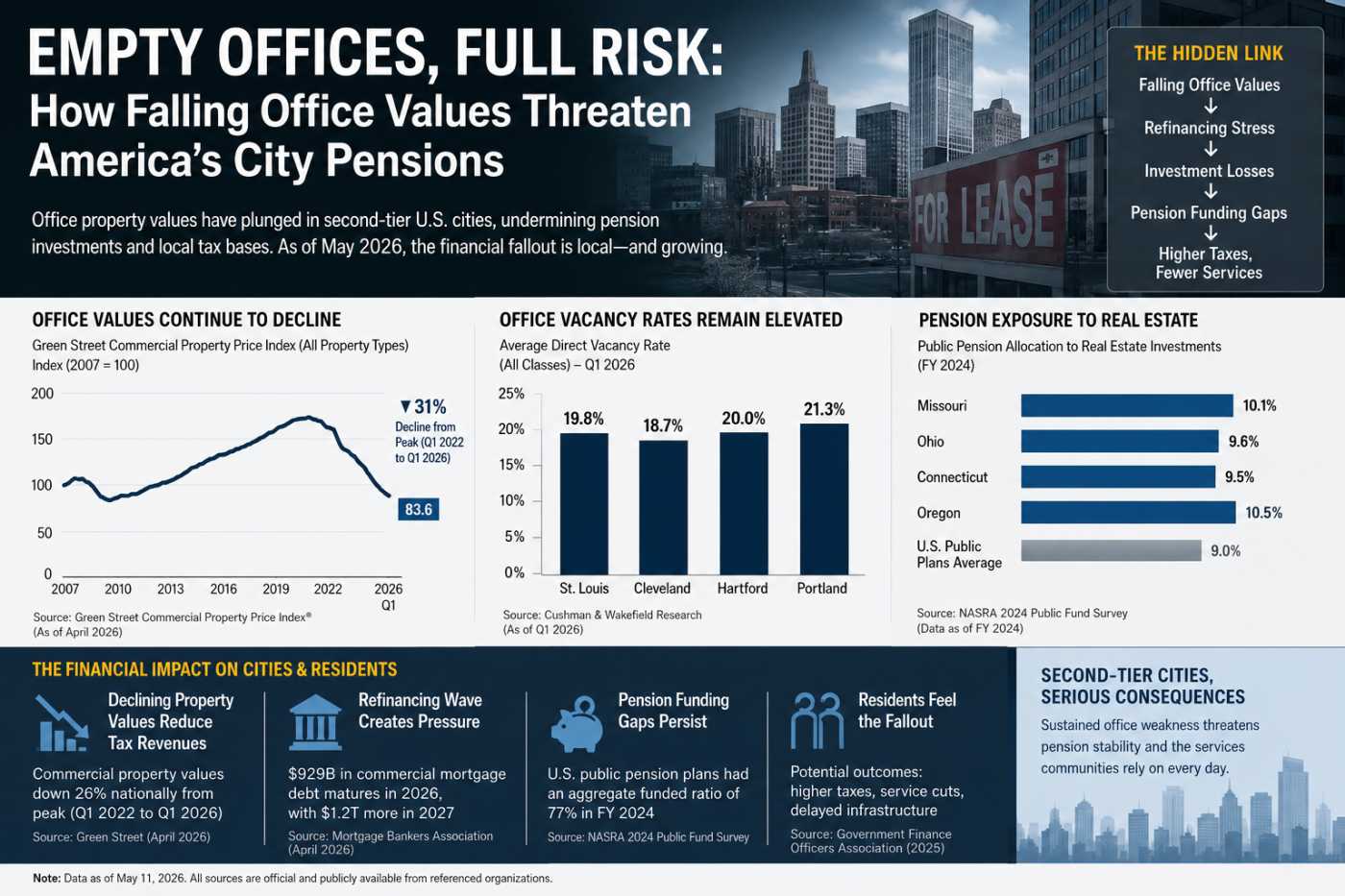
America’s Empty Offices Hit Pensions Hard
Rural Hospitals Buckle Under Private Equity
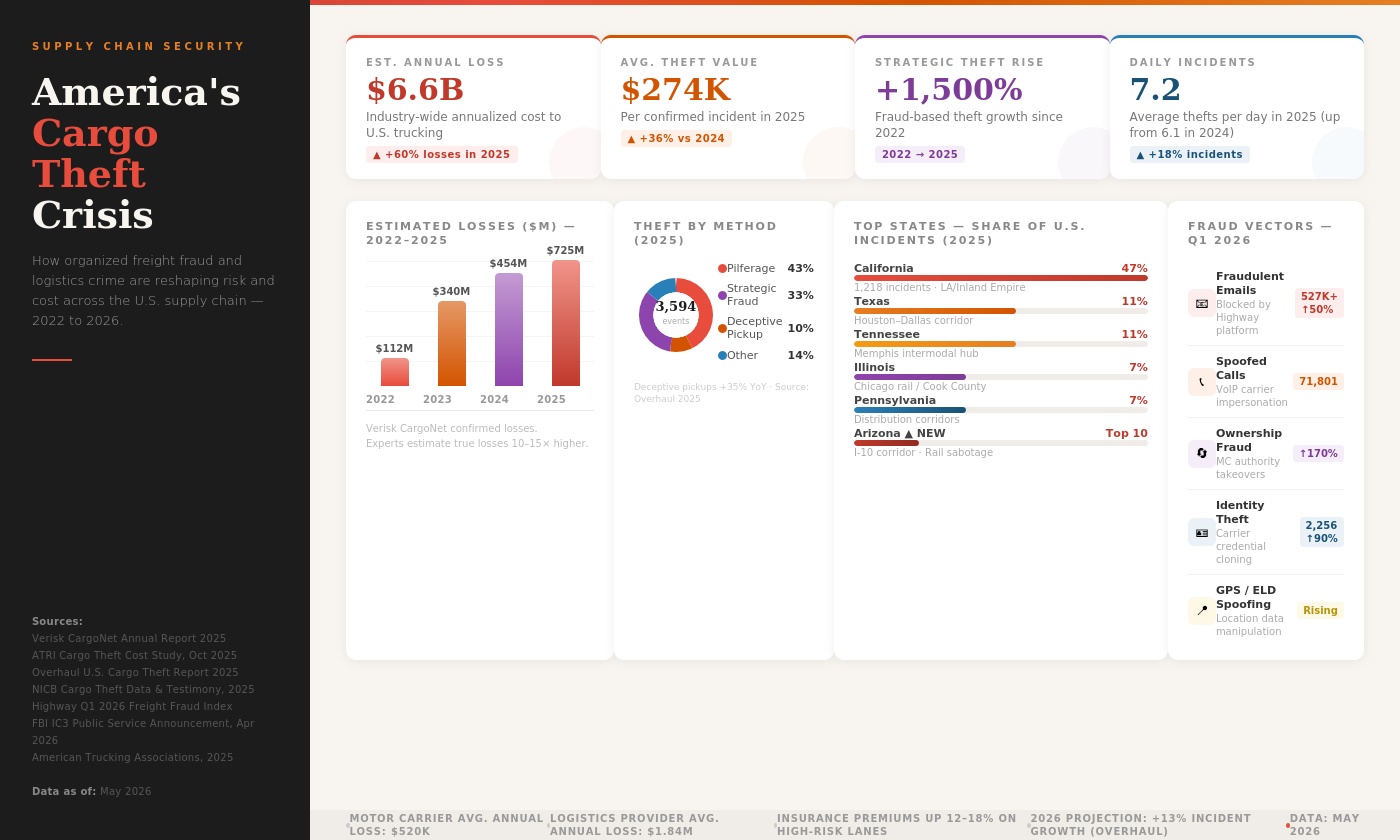
Fake Brokers, Spoofed GPS: Who Pays for Cargo Crime?
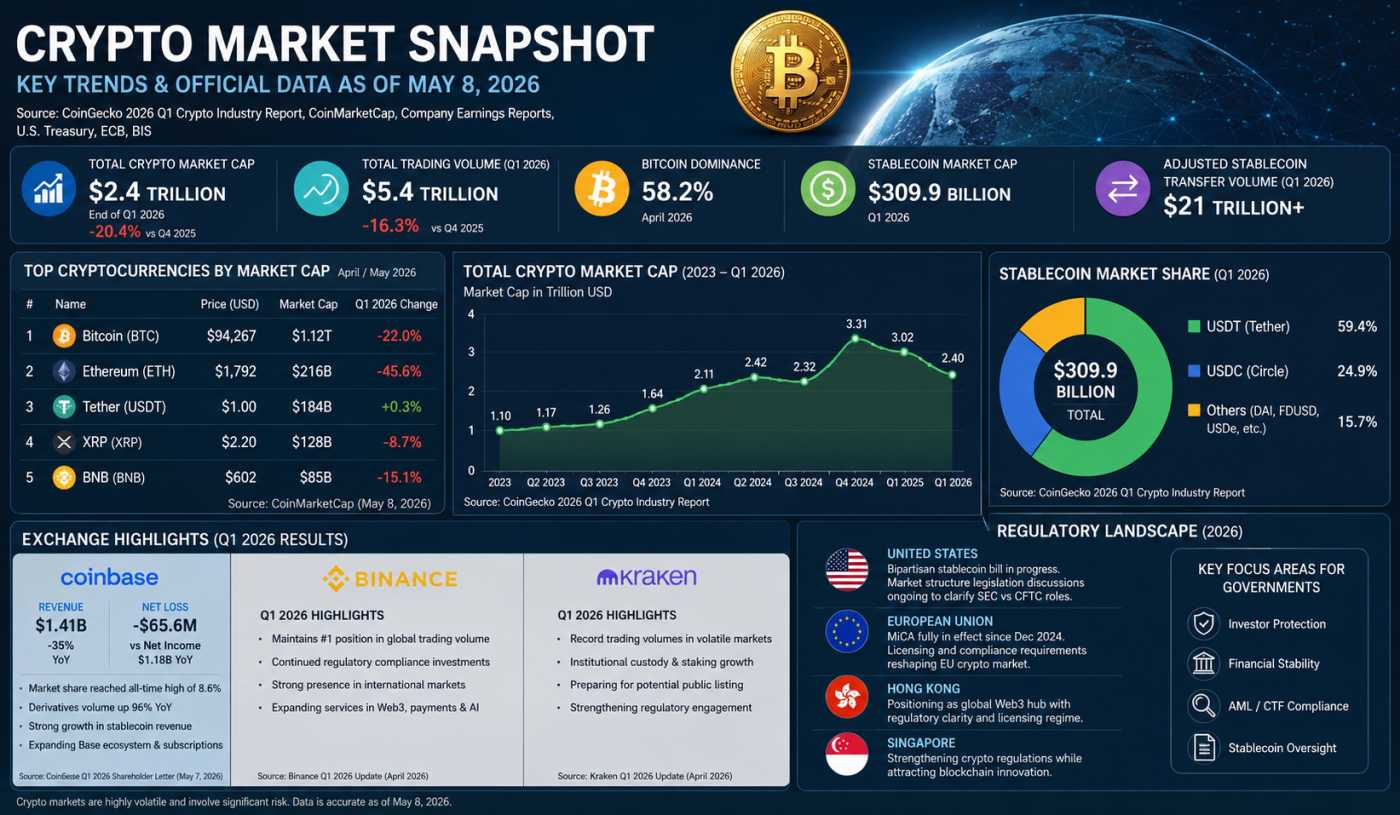
Crypto’s $2.4T Reality Check in 2026

The Machines That Ate the Grid: Five Centuries of Power Hunger
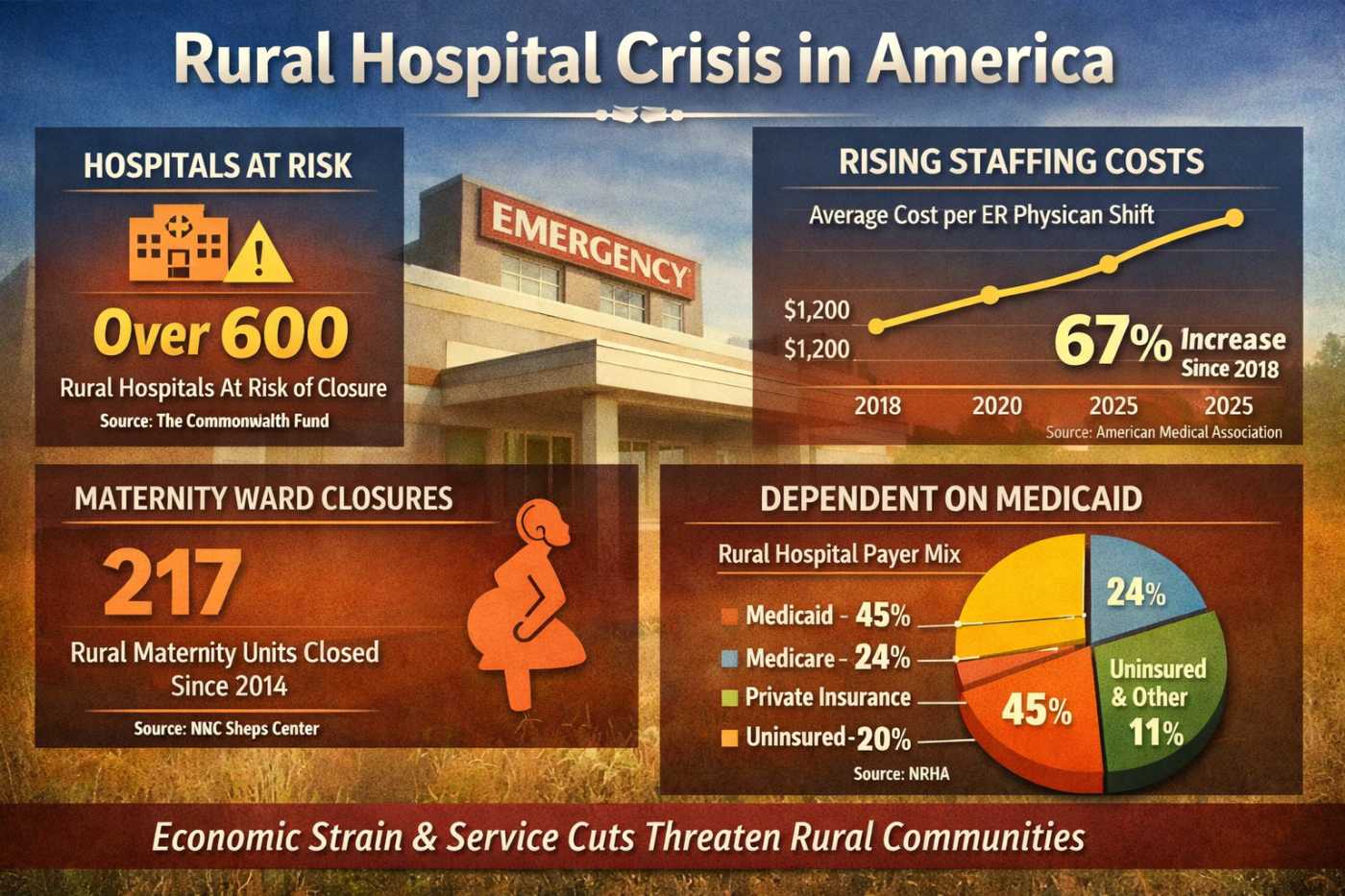
Rural Hospitals Buckle Under Private Equity



Rural hospitals across Appalachia, the Midwest, and the Deep South are facing mounting financial strain in 2026, driven by escalating staffing fees from private-equity-owned physician staffing firms and contract management groups. These pressures are worsening deficits, forcing service cuts, maternity ward closures, and delaying critical equipment upgrades, leaving communities vulnerable to losing reliable emergency care infrastructure.
Escalating Staffing Fees and Contract Pressures
Private-equity-owned emergency physician staffing firms have rapidly expanded their presence in rural hospitals. These firms often negotiate aggressively, demanding higher fees for physician coverage and emergency services. According to the Commonwealth Fund (2026), more than 20% of rural hospitals are at risk of closure, with staffing costs cited as a primary driver of operating deficits. Contract management groups frequently leverage their scale to impose terms that small hospitals cannot easily resist, further eroding margins. In some Appalachian counties, staffing fees have risen by 15–20% over the past three years, outpacing reimbursement growth and leaving hospitals unable to balance budgets.
Debt-Loaded Ownership Structures
Private equity firms typically acquire hospitals or staffing companies using debt-heavy structures. As noted by Jake Young in the American Medical Association Journal of Ethics (2025), these firms aim for rapid returns, often within 3–7 years, prioritizing profit margins over long-term stability. The debt burden is transferred to hospitals through higher service fees, leaving facilities with little room to invest in infrastructure or patient care. This financial engineering exacerbates fragility in regions already struggling with low patient volumes and high poverty rates. In the Midwest, hospitals report that debt service obligations tied to staffing contracts consume up to 12% of annual operating budgets, crowding out investment in new technology.
Impact on Hospital Operations
Operating deficits have forced hospitals to make difficult choices. In Appalachia, maternity wards have been among the first services cut, as low birth volumes fail to offset fixed staffing and equipment costs. The Commonwealth Fund reported that by 2024, one-third of U.S. counties lacked obstetric providers or birthing facilities. In the Midwest, chemotherapy and other specialized services have been discontinued in over 400 rural hospitals between 2014 and 2023, forcing patients to travel long distances for care. In the Deep South, delayed equipment upgrades such as outdated imaging machines have compromised diagnostic capabilities, further widening health disparities. Hospitals in Mississippi report average delays of 5–7 years in replacing MRI machines, compared to 2–3 years in urban centers.
Local Labor Shortages
Rural hospitals face persistent labor shortages, particularly among nurses and specialized physicians. Workforce attrition is worsened when hospitals cut services, as clinicians often leave for urban centers offering more stable employment. The shortage of local talent increases reliance on contract staffing firms, perpetuating the cycle of rising costs and financial instability. According to the National Rural Health Association (2025), rural hospitals face vacancy rates of 20% for nursing positions, nearly double the national average. This shortage forces hospitals to pay premium rates for temporary staff, further straining finances.
Medicaid Reimbursement Dependence
Rural hospitals disproportionately depend on Medicaid reimbursements, which are often lower than private insurance payments. As pandemic-era Medicaid provisions unwind, millions of rural residents risk losing coverage, according to Goldman Sachs Asset Management (2026). This reduction in reimbursement revenue compounds the financial strain, leaving hospitals unable to cover fixed costs. In states that did not expand Medicaid, the problem is particularly acute, with uncompensated care rising sharply. For example, hospitals in Alabama report uncompensated care costs increasing by 12% between 2023 and 2025, eroding already thin margins.
Economic Consequences for Communities
The closure or downsizing of rural hospitals has profound economic consequences. Hospitals are often among the largest employers in rural counties, and their loss reduces local job opportunities, weakens tax bases, and discourages new business investment. Communities without reliable emergency care infrastructure face higher mortality rates, increased travel costs for patients, and declining property values. The ripple effects extend beyond healthcare, undermining long-term economic resilience in already fragile regions. In Appalachia, counties that lost hospitals between 2010 and 2020 saw average declines of 6% in local employment and 8% in small business formation, according to the U.S. Government Accountability Office (2025).
Regional Case Studies
- Appalachia: Hospitals in West Virginia and Kentucky have reported maternity ward closures due to unsustainable staffing costs. Families must travel up to 90 miles for delivery services, increasing risks for maternal and infant health. In eastern Kentucky, Pike County’s hospital closure of its obstetrics unit in 2025 forced over 1,200 births to be redirected to distant facilities.
- Midwest: In states like Iowa and Missouri, rural hospitals have delayed upgrades to diagnostic imaging equipment, leading to slower detection of chronic conditions such as cancer and heart disease. A Missouri hospital reported that outdated CT scanners contributed to a 15% increase in delayed diagnoses between 2022 and 2025.
- Deep South: Mississippi and Alabama hospitals have faced aggressive contract renegotiations from staffing firms, resulting in fee hikes that push facilities into deficit. Service cuts have included dialysis and chemotherapy units, leaving patients with few local options. In rural Alabama, dialysis patients now travel an average of 70 miles for treatment, raising transportation costs and worsening health outcomes.
Long-Term Outlook
Without intervention, the financial pressures from private-equity-owned staffing firms and contract management groups will continue to destabilize rural healthcare. The combination of escalating fees, debt-loaded ownership structures, and Medicaid reimbursement dependence creates a fragile ecosystem where hospitals struggle to survive. The long-term economic consequences for communities losing emergency care infrastructure are severe, with diminished health outcomes, weakened labor markets, and declining regional competitiveness.
As of May 2026, the evidence from organizations such as the Commonwealth Fund, the American Medical Association Journal of Ethics, the National Rural Health Association, and Goldman Sachs Asset Management underscores the urgent need to address the financing realities of rural healthcare. The sustainability of these hospitals is not merely a healthcare issue but a cornerstone of local economic stability across Appalachia, the Midwest, and the Deep South.
If you have enjoyed reading, spread the word:
Private Credit’s Secret Banking Backbone Is Growing Faster Than Anyone Expected

America's $5 Trillion Business Handoff Has Already Begun

The Repair Economy Boom in Rural America
Debt, Deficits & Disaster: The Bond Market Crisis
