Good prospects:
Latest Regulatory Filings for NSE500
Companies with the best and the worst technicals.

NITI Blueprint Could Turn Brain Drain Into $135Bn Engine
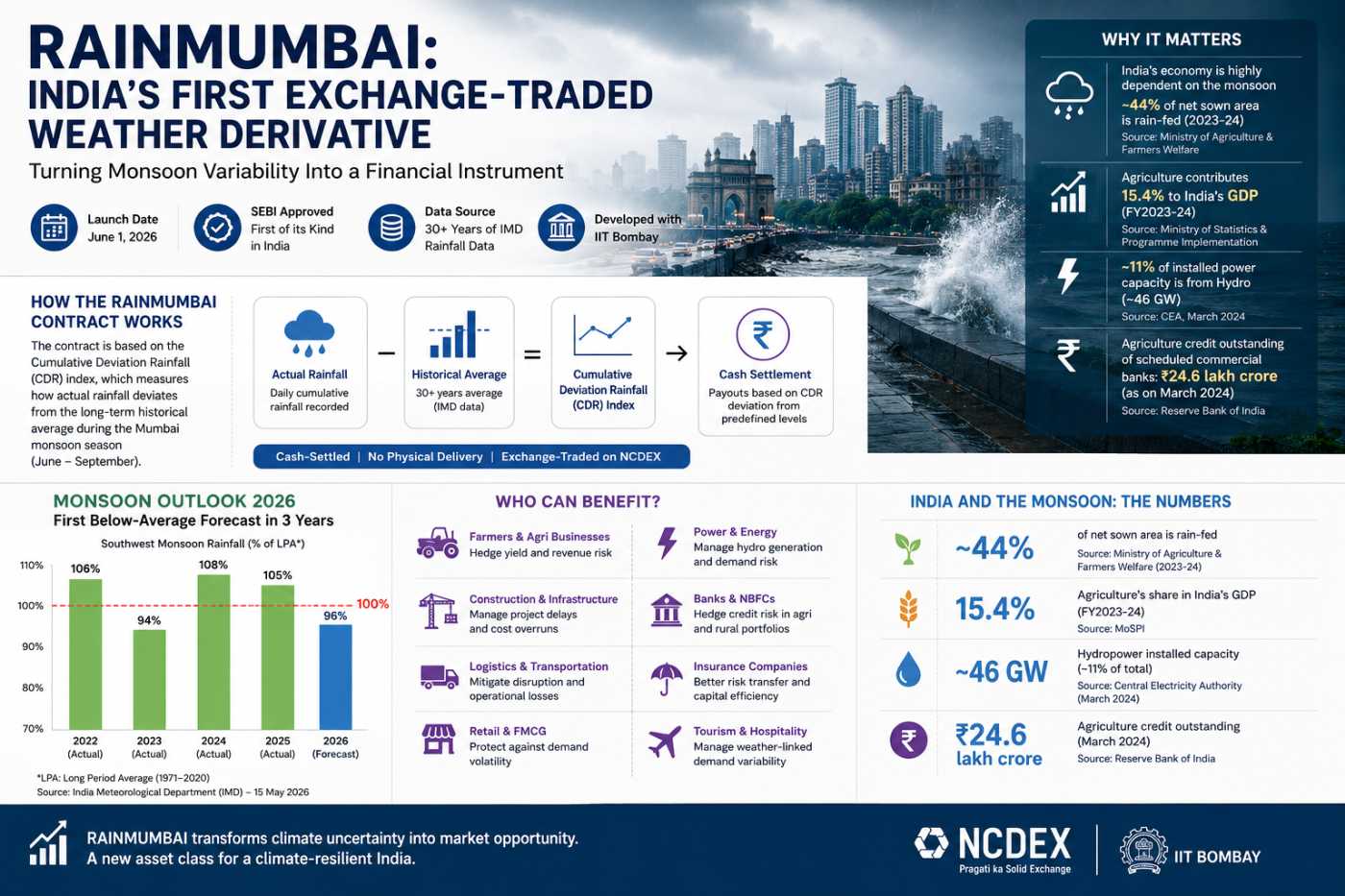
RAINMUMBAI Turns Rain Into a Financial Asset

India’s IT Sector Faces a Historic Breaking Point

How Independent Directors Failed Rs 2,500 Crore in Value

India’s Stock Market May Be Sitting on a Trap
Apollo FY26: When Healthcare Becomes a Flywheel



When Apollo Hospitals reported its FY26 results on May 20, 2026, the numbers were striking by any measure: consolidated revenue of ₹25,229 crore, up 16% year-on-year; net profit of ₹1,942 crore, a 34% leap from FY25's ₹1,446 crore; and EBITDA expanding 25% to ₹3,769 crore. Q4 FY26 alone delivered a 36% jump in net profit to ₹529 crore on revenues of ₹6,605 crore. These are not merely the results of a well-run hospital. They are the financial signature of a business model undergoing a fundamental structural transformation one that has implications far beyond healthcare.
For long-horizon investors, India's organised hospital sector is increasingly beginning to resemble something more familiar: a compounding consumer franchise. The question is not whether the numbers are good. It is whether India is, in the process of building world-class healthcare businesses, also building the world-class healthcare infrastructure the country actually needs. The answer, as it turns out, may be more nuanced than either the bulls or the critics suggest.
The Three Tailwinds That Are Structural, Not Cyclical
The first and most important tailwind is the explosive growth of health insurance. According to data cited in an April 2026 Insurance Business report on IRDAI's formation of a new subcommittee to review private health insurance, health insurance premiums in India grew 27.17% year-on-year in January 2026 alone to ₹5,414.54 crore. Health insurance is now the single largest segment within India's non-life insurance industry, contributing 41.42% of gross direct premiums in 2024–25, according to IRDAI's own annual report. The total health premium has grown from ₹20,096 crore in 2014–15 to ₹1,17,505 crore in 2024–25 nearly a six-fold increase in a decade, covering 58.20 crore lives.
This matters for hospitals because insurance transforms the demand curve. When a patient pays out-of-pocket, price sensitivity is acute and consumption is suppressed. When an insurer pays, both volumes and the willingness to opt for more complex, higher-value procedures increase. Apollo's own results confirm this: average revenue per occupied bed (ARPOB) in its healthcare services business rose 12% year-on-year to ₹71,206 in Q4 FY26, not simply because beds filled up faster, but because the case mix is shifting toward oncology, neurosciences, organ transplants, robotic surgeries, and cardiac procedures exactly the high-acuity work that insurance facilitates and that organised tertiary hospitals alone can perform.
The second tailwind is the ongoing formalisation of India's diagnostics sector. According to a CareEdge Ratings industry analysis, the organised segment still accounts for only 15-20% of India's total diagnostics market with roughly 80-85% of the industry composed of unorganised regional businesses. This is simultaneously a market inefficiency and an extraordinary growth runway. National chains like Dr. Lal PathLabs, Metropolis Healthcare, and Apollo Diagnostics are consolidating aggressively: Metropolis acquired Core Diagnostics for approximately ₹246.8 crore in December 2024, and Dr. Lal PathLabs added 18 new laboratories and nearly 900 sample-collection centres in FY25 alone. Emkay Research forecasts Metropolis Healthcare to grow Q4 FY26 revenue by 24%, and Vijaya Diagnostic Centre by 20% year-on-year. NABL accreditation is increasingly becoming a prerequisite for insurance empanelment, structurally disadvantaging unorganised labs and accelerating consolidation in favour of listed players. Diagnostics, in other words, is at the precise inflection point that retail pharmacy was a decade ago.
The third tailwind is premiumisation not just of procedures, but of the entire healthcare consumption experience. India's healthcare costs are rising at approximately 14% annually, significantly outpacing general inflation, according to PS Market Research's India Health Insurance Market report. Non-communicable diseases cardiac conditions, cancer, diabetes, hypertension now account for over 60% of India's total disease burden. These are chronic, recurring conditions that require continuous monitoring, specialist interventions, and long-term pharmaceutical management. Apollo's MD Suneeta Reddy has explicitly noted this shift in the company's strategic orientation: "Apollo Hospitals is pivoting toward preventive healthcare as non-communicable diseases account for over 60% of India's total disease burden." This is not simply a public health narrative it is a business model insight. Chronic disease is a recurring revenue model. Episodic acute care is not.
The Flywheel That Is Beginning to Spin
What makes Apollo's FY26 results particularly instructive is not the headline numbers but the ecosystem logic they reveal. The company now operates across at least five distinct but interconnected layers: tertiary hospitals, retail pharmacies (7,289 outlets as of March 2026), the Apollo 24/7 digital health platform, Apollo Diagnostics, and Apollo Health and Lifestyle (AHLL), its retail health and diagnostics subsidiary.
Apollo HealthCo the entity that houses the pharmacy and digital health operations posted FY26 revenue of ₹10,808 crore, up 19% year-on-year, and critically, reported its first full year of profitability. Apollo 24/7's gross merchandise value crossed ₹2,037 crore in FY26, with daily order run-rates reaching approximately 69,000 orders across pharmacy, diagnostics, and consultations in Q4 alone. Apollo Health and Lifestyle posted 20% revenue growth while narrowing its losses. These are not vanity metrics. They represent the early operational evidence of a flywheel: a patient who consults on Apollo 24/7 is nudged toward an Apollo diagnostic centre, fills their prescription at an Apollo pharmacy, and is eventually referred to an Apollo hospital for a complex procedure. Every touchpoint reinforces every other touchpoint.
This vertical integration strategy mirrors with important differences the playbook that India's leading FMCG conglomerates executed in the 1990s. HUL, ITC, and Marico built distribution moats first, then extended into adjacent categories, using the trust and reach of established brands to lower customer acquisition costs in new segments. Apollo is doing the same, but in reverse: the hospital brand creates clinical trust, which then flows downstream into pharmacy, diagnostics, and digital. The ARPOB expansion, the pharmacy store additions, the diagnostics volume growth these are individually meaningful, but their combined network effect is the real story.
The Demerger: Unlocking Value, Raising Questions
Perhaps the most consequential structural move Apollo has made in recent years is its planned demerger of Apollo HealthCo encompassing Apollo 24/7, the pharmacy distribution business, and Keimed into a separately listed entity by Q4 FY27. The combined entity is projected to generate approximately ₹25,000 crore in revenue at listing, with management targeting 20% annual growth against 18% for the hospitals business. Apollo Group CFO Krishnan Akhileswaran has confirmed the company is on track, pending approvals from SEBI, NCLT, and stock exchanges.
The strategic logic is sound: a pharmacy and digital health platform deserves a consumer-tech valuation multiple, not a hospital EBITDA multiple. Separating the two businesses allows each to be valued and funded on its own terms, and potentially unlocks significant shareholder value. Apollo Hospitals' stock jumped over 4% to a record high when the demerger was announced, reflecting market enthusiasm for the move.
But the demerger also raises a structural question that the investment community has not fully interrogated: once the flywheel is disaggregated into two separately listed entities, does the ecosystem logic hold? The compounding value of vertical integration depends on seamless data flows, cross-referral economics, and shared patient relationships. A separate listing creates independent boards, separate capital allocation priorities, and potential misalignments. Apollo's leadership, particularly Shobana Kamineni, has stated that the omnichannel model will remain operationally integrated even after legal separation. Whether that commitment survives the accountability structures of two independent listed entities each with its own shareholder base and analyst community remains a genuine open question.
CareEdge's 11-12% CAGR Forecast and What It Really Means
A January 2026 report by CareEdge Ratings projected India's hospital sector to grow at 11-12% CAGR on the back of rising insurance coverage, medical tourism demand, and private sector expansion. In 2024, over 700,000 medical tourists visited India primarily from Africa, West Asia, and South Asia drawn by clinical outcomes that increasingly rival Western centres at a fraction of the cost. Apollo's FY26 results confirmed this: international patient revenues maintained momentum, aided by partnerships with governments, embassies, and healthcare information centres across Africa, the Middle East, Bangladesh, and Southeast Asia.
The 11-12% CAGR projection, in context, implies that Apollo and its organised peers Max Healthcare, Fortis, Narayana Hrudayalaya, Aster DM Healthcare are not growing because healthcare demand in India is growing moderately. They are growing because they are capturing a disproportionate share of a large, previously unorganised market. The hospital sector's structural dynamics today resemble the private banking sector of the early 2000s: total market size was large but fragmented, organised players had structural cost and quality advantages, and the expansion of formal credit (or in this case, formal insurance) was the catalyst that allowed organised players to take share at scale. HDFC Bank, Kotak, and ICICI compounded for decades on the back of that dynamic. The question for Apollo, Max, and Fortis is whether organised healthcare can do the same.
The Uncomfortable Question That Deserves a Serious Answer
India's out-of-pocket healthcare expenditure still accounts for approximately 39.4% of total health expenditure, according to Press Information Bureau data a figure that, while declining, remains one of the highest among comparable middle-income economies. The very insurance-driven premiumisation that is powering Apollo's ARPOB growth and margins simultaneously pushes the cost of sophisticated care further out of reach for uninsured or underinsured populations. When Apollo opens a 400-bed smart hospital in Hyderabad's Financial District as it did in April 2026 it is serving a different India than the one that accounts for the bulk of the country's disease burden.
Apollo Group Chairman Prathap C Reddy has framed the company's Tier-II and Tier-III expansion as a response to this tension: "Our expansion strategy continues to be guided by India's long-term healthcare needs. This is not only a strategic priority, but also a responsibility to bring advanced healthcare closer to underserved communities while maintaining the highest standards of care." New facilities in Sonarpur, Kolkata, were commissioned alongside the Hyderabad flagship in FY26, and the group's total bed network stood at 8,131 as of March 2026.
The honest answer to the question is India building world-class healthcare infrastructure or world-class healthcare businesses? is that it is building both, but not at the same pace, for the same populations, or with the same urgency. The organised private sector is building exceptional, financially compounding institutions. The infrastructure needed to serve the bottom half of India's population health needs remains structurally dependent on government scheme coverage, public hospital capacity, and the reach of insurance schemes like Ayushman Bharat. These are not contradictions so much as parallel tracks moving at different speeds. For investors, the organised private sector story is compelling, durable, and structurally supported. For policymakers, the question of who ultimately pays for India's healthcare transformation and who benefits from it remains as open as ever.
Apollo Hospitals' FY26 results are a data point in a much larger story. That story is not simply about one company, or even one sector. It is about the financialisation of Indian healthcare and what it means when a country's most essential public good becomes its most attractive private compounding machine.
If you have enjoyed reading, spread the word:

Beyond Sugar: India's Bio-Economy Bets Big on Biofuel
MSMEs & Corridors: India's New Economic Engine
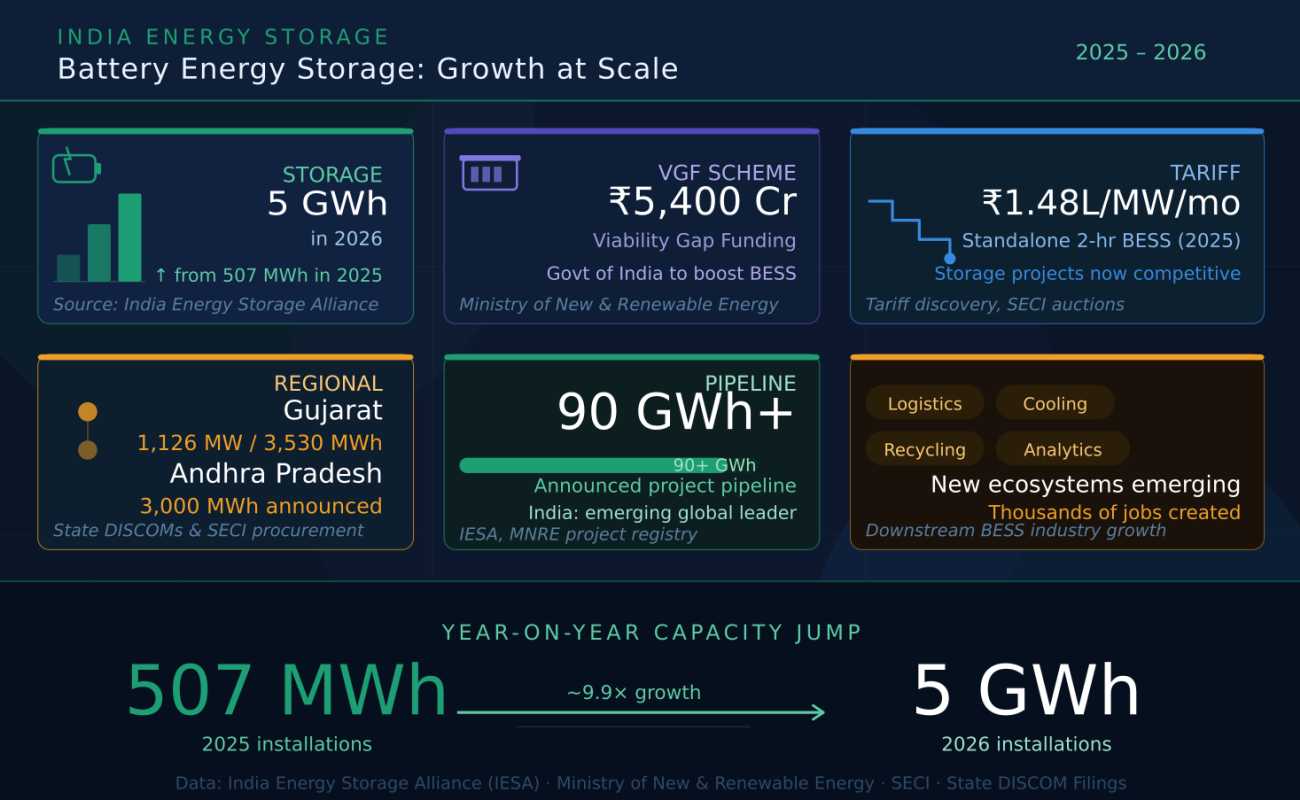
India's Grid-Scale Storage Revolution 2026

Why Gujarat And Rajasthan Are Winning Big
